it is characterized by mostly motor symptoms and sometimes non-motor symptoms. for motor it includes muscle rigidity, bradykinesia, resting tremor and balance issues. non-motor symptoms include constipation, hallucinations, mood disorders, pyschosis, sleep disturbances and fatigue.


for healthy humans, dopaminergic neurons release an amount of dopamine sufficient to control the stimulating effect of acetylcholine on large motor and fine muscle movements. dopamine and acetylcholine are balanced. but in humans with Parkinsons, the dopaminergic neurons in the brain are progressively and irreversibley destroyed which causes dopamine deficiency, a relative decrease in inhibitory dopamine and an increase in excitatory acetylcholine in the brain causes excessive motor stimulations. now acetylcholine is higher than dopamine.

drug therapy: the goal is to increase inhibitory dopamine activity or decrease excitatory acetylcholine activity. this restores the balance of the two and restores dopaminergic activity by increasing the levels of levodopa which is a precursor to dopamine that crosses the blood brain barrier (BBB). But once its in the brain it gets converted to dopamine to replace deficiency caused by damaged neurons. another way is using dopamine agonists. and restoring normal balance of cholinergic drugs aka anti-muscarinic drugs. the treatment is NOT a cure but rather improves symptoms and quality of life. dopamine goes under rapid metabolism in the GI tract and liver so it does not cross the BBB therefore cannot be given orally. levodopa mentioned earlier (L-dopa) it does get absorped orally but as said before it can be metabolized to dopamine on either side of the BBB in the peripheral nervous system and CNS. reducing the metabolism in the peripheral circulation ensures more levodopa gets to the brain. so levodopa gets combined with an enzyme inhibitor DOPA decarboxylase inhibitor like carbidopa to prevent that metabolism under after levodopa crossed the BBB and once it does levodopa is metabolized to dopamine and supplements the low levels of dopamine.
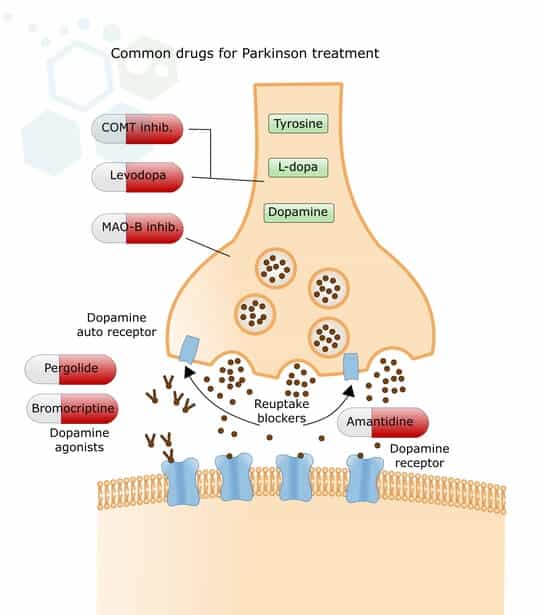
drugs for PD: levodopa and carbidopa are sold in a fixed combination called Sinemet and Sinemet CR the CR is the controlled release formulation, since this medication needs to be taken multiple times a day it can disturb the patients sleep so the CR version was created. the dose may need to be decreased over time to avoid adverse effects, there is also less repsonse over time so drug holidays can help. Sinemet is available as 100mg/10mg, 100mg/25mg and 250mg/25mg. the CR version comes in 100mg/25mg and 200mg/50mg. another drug is dopamine receptor agonists they mimic dopamine by binding to the receptors and activate them. those drugs are Pramipexole (Mirapex) and Ropinirole (Requip) they can be used alone or in combo with levodopa-carbidopa, it starts at a low dose and is increased overtime. another type of drug is MAO-B inhibitors, Monoamine oxidase-B is an enzyme in the body that breaks down dopamine. they've been used to treat depression, it metabolizes norepinephrine, serotonin and dopamine, it also metabolizes dopamine selectively. Selegiline is well tolerated and at high dose inhibits MAO-A. next is COMT catechol-O-methyl transferase which is an enzyme that breaks down levodopa, decrease in peripheral metabolism of levodopa and increase of levodopa. Entacapone increases the effect of levodopa/carbidopa, it is available alone or comes in a combo called Stalevo (pictured below). Anticholinergics are another one, benztropine and procyclidine block muscarinic receptors, used in combo with levodopa. it improves tremors, decreases drooling and drug-induced extra-pyramidal symptoms (EPS). the CR versions cannot be crushed some may be halved and regular formulations should be taken on an empty stomach.
