

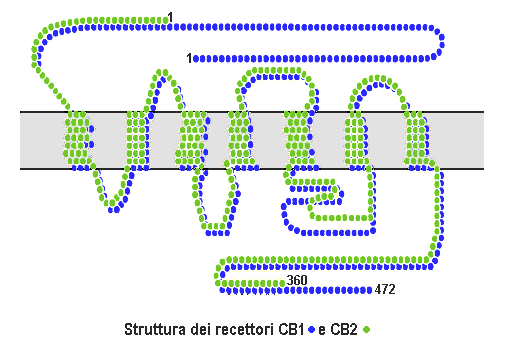
The receptors were discovered in in vitro studies during the 1980’s with that receptor becoming cannabinoid receptor type 1 or CB1. The DNA sequence that encodes the cannabinoid receptor in the human brain was found and then cloned in 1990, then in 1993 after this discovery the second brain cannabinoid receptor was created named cannabinoid receptor type 2 or CB2. There is a possible neurotransmitter for the endocannabinoid system in the brain and PNS was anandamide, first characterized in 1992 followed by other discoveries of fatty acid neurotransmitters that also behave as an endogenous cannabinoid by having a low-to-high range of efficacy for stimulating the CB1 and CB2 receptors.
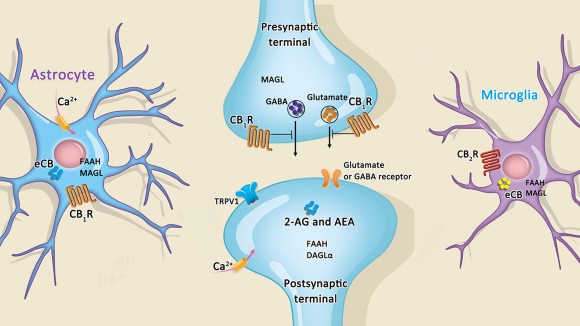
Now onto the types, first is Cannabinoid receptor type 1 aka CB1. They are thought to me the most expressed inhibitory G protein alpha subunit protein coupled receptors in the brain. One mechanism they use to function is the endocannabinoid mediated depolarization induced suppression of inhibition which is a short-term synaptic plasticity form where neuron depolarization causes a temporary reduction in GABAergic inhibitory input. It is a retrograde signaling process, where released endocannabinoids travel backwards to activate the presynaptic CB1 and CB2 receptors which reduces GABA release. Endocannabinoids that are released from the depolarized post-synaptic neuron bind to the CB1 receptors in the pre-synaptic neuron and in result causes a reduction in GABA release due to limited presynaptic calcium ions entry. Since they are found in other parts of the body like the liver, the activation of CB1 is know to increase de novo lipogenesis (DNL) which is metabolizing excess dietary carbohydrates into new fatty acids.
For Cannabinoid receptor type 2 aka CB2 are expressed on the T cells in the immune system, B cells, macrophages, hematopoietic cells, the brain and CNS. They also function in keratinocytes which are cells found in the epidermis, they have also been expressed on peripheral nerve terminals. They play a role in antinociception which is the relief of pain (analgesic). In the brain they are mostly expressed by microglial cells though that role remains unclear. The most likely cellular targets and executors are immune derived cells like leukocytes. The existence of a third receptor has long been talked about due to the actions of abnormal cannabidiol (Abn-CBD) that produces cannabinoid-like effects on blood pressure and inflammation but doesn’t activate CB1 or CB2.
Signaling! The cannabinoid receptors are activated by cannabinoids which are made naturally in the body aka endocannabinoids. Or can be introduced through the body as cannabis. After the receptor is engaged there are these pathways called intracellular signal transduction which get activated. At first it was thought that the cannabinoid receptors are mainly inhibited the enzyme Adenylate Cyclase and positively influenced inwardly rectifying potassium channels. There is now a more complex picture in different cell types which implicate other potassium ion channels, calcium channels, protein kinase A and C, and many more. The primary leukocyte CB2 displays a complex signaling profile which activates the adenylate cyclase via stimulatory Gs alpha subunit alongside the Gi protein alpha subunit. Which induces extracellular signal=regulated kinases (ERK), p38 mitogen-activated protein kinases and pCREB pathways. The separation between therapeutically undesirable psychotropic effects and the clinically desirable effects were not reported in agonists that bind to cannabinoid receptors. THC, anandamide and 2-arachidonylglycerol produce most of their effects by binding to both CB1 and CB2.
 What are the treatments? Synthetic THC (tetrahydrocannabinoid) is prescribed under the name dronabinol (Marinol) to treat vomiting and improve appetite. Many AIDS patients use this as well as people suffering from CINV. THC is also an active ingredient in nabiximols (Satviex) which is a specific extract of cannabis that was approved as a botanical drug in the UK as a mouth spray for patients with multiple sclerosis to help with neuropathic pain, overactive bladder and spasticity.
What are the treatments? Synthetic THC (tetrahydrocannabinoid) is prescribed under the name dronabinol (Marinol) to treat vomiting and improve appetite. Many AIDS patients use this as well as people suffering from CINV. THC is also an active ingredient in nabiximols (Satviex) which is a specific extract of cannabis that was approved as a botanical drug in the UK as a mouth spray for patients with multiple sclerosis to help with neuropathic pain, overactive bladder and spasticity.