
the gastrointestinal tract is a series of hollow organs joined in a long twisting tube from the mouth to the anus. there are a lot of disorders and disease of the gastrointestinal system but i learned some more common disorders today. acid reflux, GERD, bowel disease/disorders, diarrhea and nausea and vomiting.
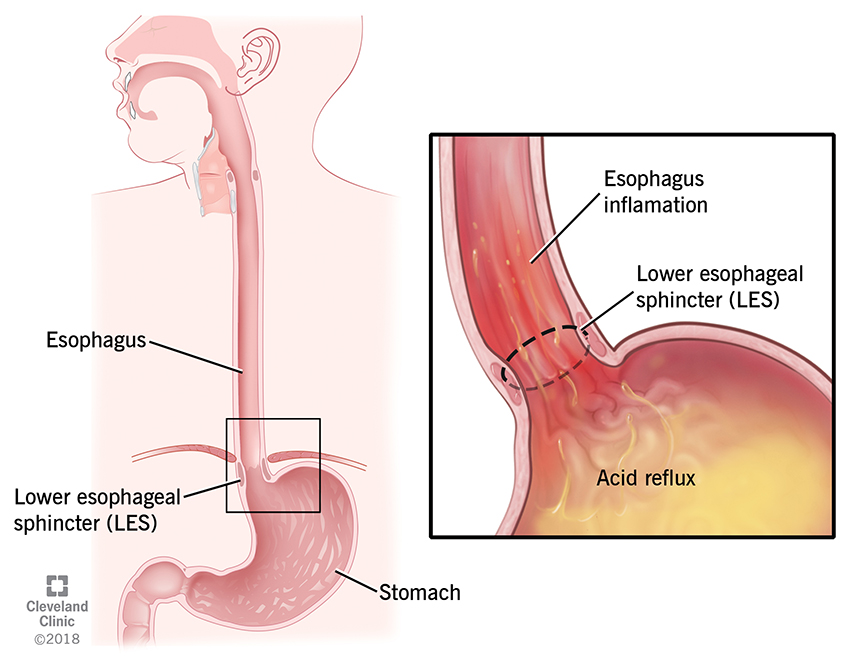
what is acid reflux and GERD? acid reflux is the movement of stomach acid going into the esophagus it can happen after eating a large meal or lying down after eating. It's an occasional disease. while GERD on the other hand is a chronic disease, it stands for Gastro Esophageal Reflux Disease. it's also the movement of stomach acid into the esophagus but happens at least twice a week for several weeks. both acid reflux and GERD have heartburn as symptoms acid reflux also has indigestion. GERD has more symptoms like a sore throat, coughing and shortness of breath (SOB). the causes of these 2 disease is because of the lower esophageal sphincter (LES) which is a ring of muscle that forms a valve, located between the esophagus and stomach. the function is to prevent backflow of acid. we predict that the LES is weakened which is causing the acid backflow and symptoms of heartburn. other causes are eating large meals, being overweight, smoking, being pregnant, some medications can also cause these issues. the most used drug treatments for acid reflux and GERD include lifestyle changes, Antacids, histamine-2-receptor antagonists (h2-blockers) and proton pump inhibitors (PPIs)


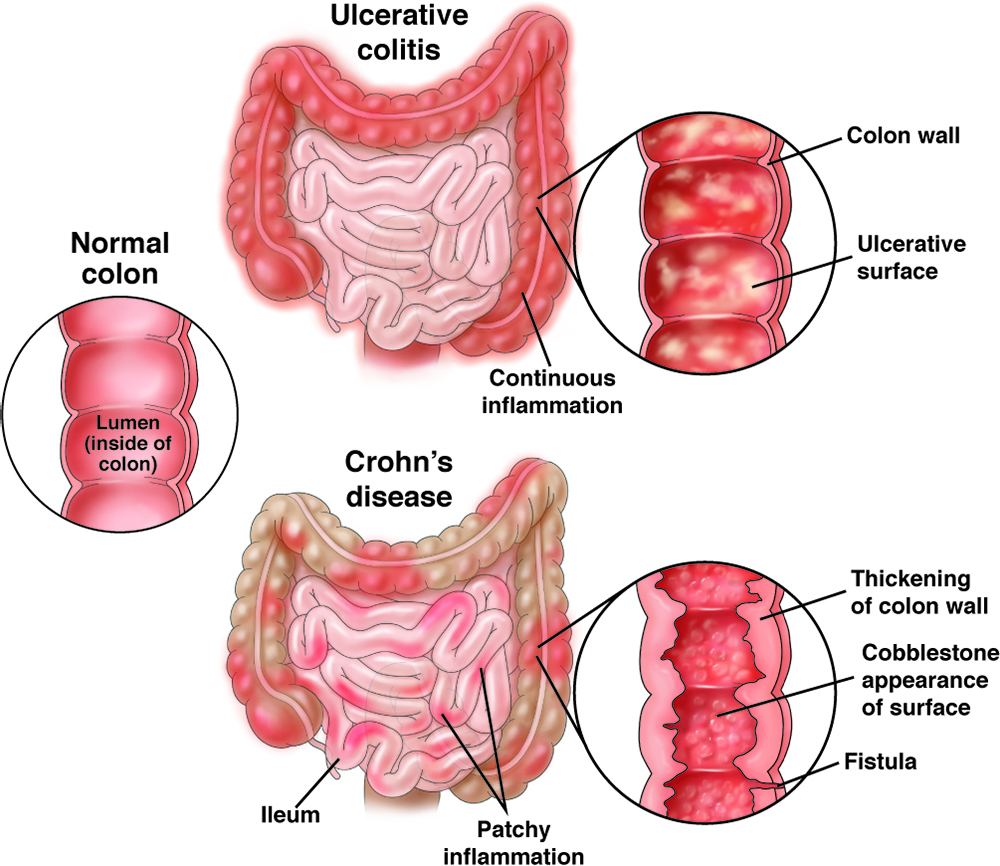
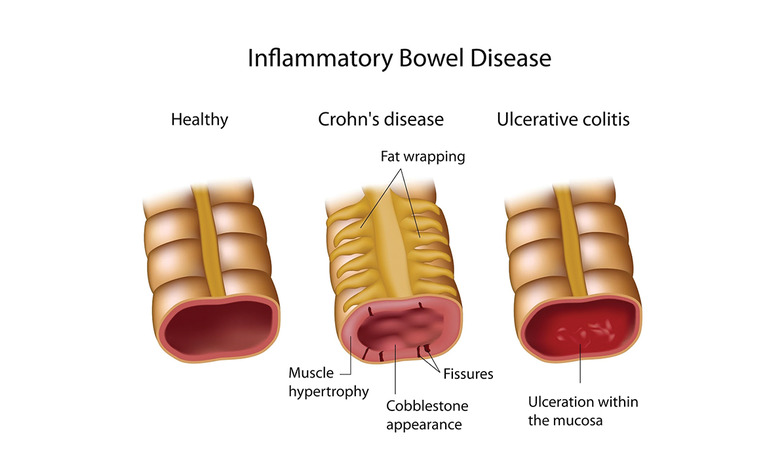
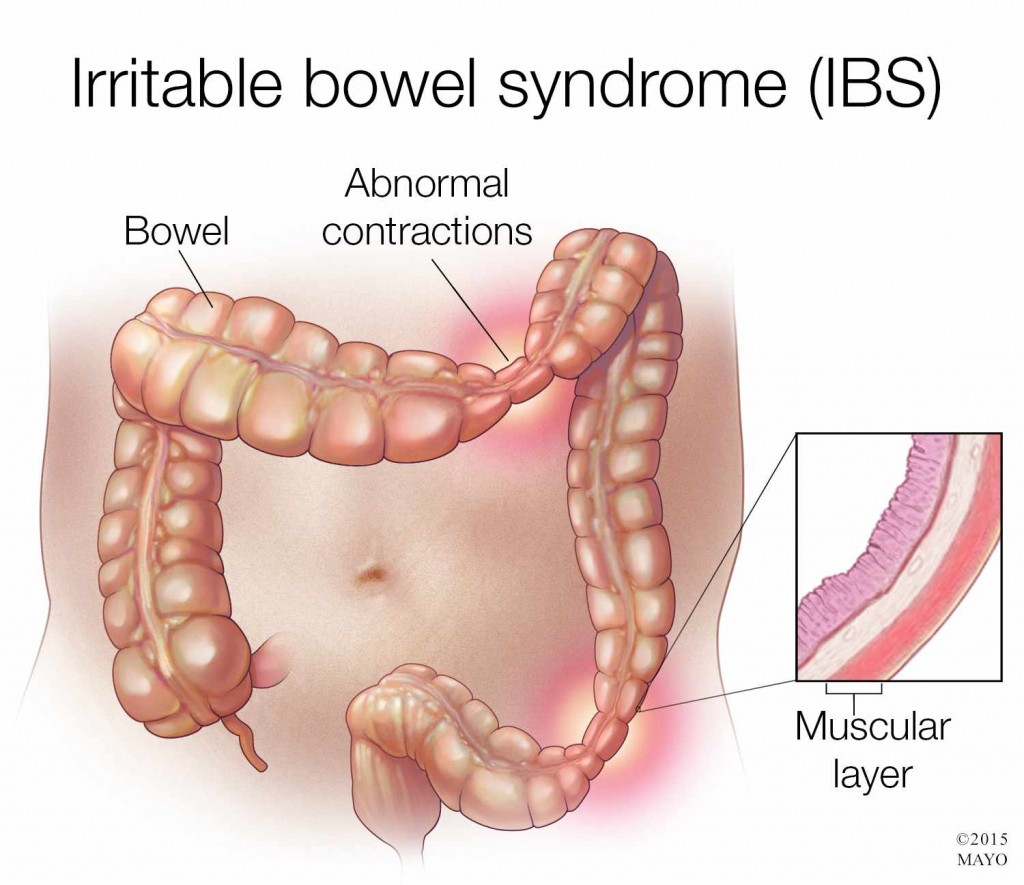
now what are the bowel disease/disorders? inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). diverticulitis and celiacs disease also fall under this category. IBD describes 2 main chronic diseases; ulcerative colitis which is most common then crohns disease. there is also indeterminate colitis which is both crohns and ulcerative colitis. ulcerative colitis can affect any part of the large intestone and rectum which causes complete damage to the inner lining only and creates ulcers, the symptoms can vary in severity it depends on how much damage and what extent of damage in the colon. blood/mucus in the stool, bowel urgency and stomach cramps are the symptoms. with crohns disease it can affect ANY part of the GI tract from the mouth to the anus, so a lot more than ulcers. it causes inflammation along the way. in the intestinal wall the inflammation can reach the outher lining which causes swelling in patches. these symptoms also depend on the severity in the GI tract, such as diarrhea that is not bloody, mouth sores and malnutrition. the causes of inflammatory bowel disease is not well understood it could be a number of things such as abnormal immune response which is when the body's immune system attacks healthy bowel cells which cause inflammation. genetics and environmental factors also play a part. because of the abnormal immune response IBD is considered an auto-immune disease. the treatment for IBD is drug treatments such as amniosalicylates (5-ASA), corticosteroids, immunomodulators, biologics and surgery like a colectomy (removal of the colon). what is IBS? irritable bowel syndrome is the disorder of the motility and sensitivity of the large intestine, a patient will experience changes in bowel patterns and abdominal pain, bowel habits can range between diarrhea and constipation. the causes of IBS is also not well understood. dysmotility which is food passing through the gut quickly, the colon contractions cause cramps and pain, sensitive nerves in the gut, family history, severe infection and food intolerance are all possible causes. IBS is considered a neurogastrointestinal disorder because of the sensitive nerves in the gut. there is no cure for IBS but there are symptom management approaches such as diet changes and lifestyle changes. the drug management approach are laxatives which relieve constipation, anti-diarrheals which control diarrhea and anti-spasmodics which treat intestinal spasms. i'm not going over diarrhea and N/V i know too much.
but lets talk about the drugs! for acid reflux and GERD we have non-rx products like antacids which work by neutralizing the acid in the stomach, they are fast acting working in 5-15 minutes. e.g. Tums, Rolaids, Maalox and Gaviscon. now Rx products! histamine-2-receptor antagonists also called H2 blockers, their drug name stem is "-tidine" such as cimetidine. they work by binding reversibly to H2 receptors which are located on the gastric parietal cells therefore reduces histamine-induced acid secretion in the stomach. they work well when taken at night. they are usually well tolerated by cimetidine is associated with headaches and gynecomastia it is also a strong CYP450 enzyme inhibitor so use with caution. Nizatidine (Axid) is a rx only H2 blocker. next we have proton pump inhibitors (PPIs) they are the first-line drug for most acid-related disorders. their stem is "-prazole" such as pantoprazole. the H+/K+ ATPase which is also known as the proton-potassium pump is a vital enzyme found in the parietal cells of the stomach lining. it plays a crucial role in the secretion of gastric acid which is essential for the digestive process. this pump is the final step in acid secretion into the stomach. the PPIs block this enzyme, so stomach acid doesn't jump up into the esophagus. PPIs represent the most potent drugs for acid reduction. but there is also cimetidine and hypomagnesemia and vitamin B12 deficiency to worry about. some products available are omeprazole (Losec) and esmoeprazole (Nexium) are non-rx too if they have a low dose and limited pack size. pantoprazole Na (Pantoloc), pantoprazole Mg (Tecta), rabeprazole (Pariet), lansoprazole (Prevacid) and dexlansoprazole (Dexilant) are all Rx-only. most PPIs are delayed-release formulations meaning the tablets contain enteric-coated granules which cannot be crushed, it's designed to be protected from gastric acid and released and absorbed from the small intestine.


interesting fact about vomiting! the 4th ventricle of the brain hosts the vomiting center and the chemoreceptor trigger zone called (CTZ). CTZ contains receptors for dopamine, serotonin and acetylcholine. when these receptors are stimulated CTZ activates the vomiting center which leads to vomiting.

treatment for IBD!! the goals of therapy is to reduce inflammation in the gut (a local effect). acute treatment of IBD or flare-ups and chronic maintenance therapy is used to prevent recurrences. this includes GI NSAIDs, SAIDs, immunosuppressants, biologic response modifiers and surgery. the choice of treatment depends on the severity if it's a flare up or remission, the area and the course of the disease. Ulcerative colitis has the pyramidal step-up approach and crohn's uses a top-down approach.
GI NSAIDs - first is aminosalicylates (5-ASA) their indication is the treatment of uncomplicated, mild to moderate ulcerative colitis (proctitis and left-sided colitis), it is considered standard/baseline therapy for ulcerative colitis (UC), it is used occasionally in crohn's disease. 5-ASA is chemically related to aspirin. the drug choices include sulfasalazine and mesalamine. sulfasalazine is a prodrug 5-ASA (drug activity) + sulfapyridine (increases side effects), it is converted by bacteria in the colon, used for UC, crohn's and rheumatoid arthritis. the brand name is Salazopyrin / Salazopyrin EN, the side effects include abdominal pain, N&V, skin rash and steven-johnson syndrome. it should be taken with food to reduce GI irritation and has to be swallowed whole and cannot be crushed or chewed. for Mesalazine the drug treatment starts with rectal suppositories, enema or a rectal foam for inducing remission of disease and then as maintenance therapy. the pryamidal step-up approach if rectal doesn't work add in topical corticosteroids then an oral 5-ASA. rectal therapy produces concentrations 100x higher at site of inflammation compared to oral therapy, therefore it is prefered in inducing remission, it comes as tablets, capsules, rectal enemas, suppositories and foams. it comes as Pentasa, Mezavant, Mezera, Octasa and Salofalk. the side effects include abdominal pain, headaches and nausea. this is also taken with food and swallowed whole bu the Pentasa capsules open them up and sprinkle it in apple sauce. Mezavant should be swallowed whole with liquid.
SAIDs - Steroidal Ani-Inflammatory Drugs: oral dosage forms are 1st line treatment of active, moderate to severe ulcerative colitis (proctitis and left-side colitis). rectal is the 2nd line treatment of mild-moderate UC who have not responded to rectal ASAs. it is used for anti-inflammatory and immune suppressive activity, it's considered ineffective when used for long term remission it is associated with many adverse effects inducing impaired glucose tolerance and osteoporosis. synthetic corticosteroids mimic glucocorticoids that body produces naturally such as cortisol or cortisone. when it is given topically for UC it is considered to be less effective than a 5-ASA rectal treatment. the drug choices include prednisone (Winpred), prednisolone (Pediapred), bethamethasone disodium phosphate (Benesol) rectal enema, budesonide (Entocort) rectal enema and hydrocortisone rectal enema (Cortenema)
immunosuppressants - the indication is used for both UC and Crohn's disease, when 1st line and 2nd line treatmetn fails to control the disease. the mechanism of action suppresses the body's immune system hence reducing inflammation. the drug choices are Methotrexate, Azathiopurine, 6-mercaptopurine, Cyclosporine and Tacrolimus. there are also biologic response modifiers aka Biologics. they are genetically engineered large, complex molecules usually proteins designed to inhibit or enhance specific components in the immune system such as tumor necrosis factor (TNF), it is approved to treat moderate to severe crohn's and UC. patients see benefits within 2-12 weeks. the common drug name stem for monoclonal antibodies is mab. they are require parenteral administration, IM or SC and some are available both IM and SC such as golimumab. there are anti-tumor necrosis factor alphas which inhibit the TNF-a which signals other cells to start the inflammatory process such as Etanercept (Enbrel), adalimumab (Humira) and golimumab (Simponi, Simponi IV), infliximab (Remicade) and it's biosimilar (Inflectra), certolizumab (Cimzia), vedolizumab (Entyvio) and ustekinumab (Stelara).